
Diversity and Inclusion
We, the Community Care Cooperative Board of Directors, hereby declare racism a public health crisis and affirm our commitment to diversity, equity and racial justice. We commit to implementing a proactive response to racial injustice, including charging management to create a Committee that will provide organizational leadership.
Our employee-led Diversity, Equity, and Racial Justice (DERJ) Committee works to acknowledge, recognize, and address how white supremacy and systemic racism have adversely impacted people and communities of color. We seek to:
Current Initiatives of the Diversity, Equity, and Racial Justice Committee
We strive for true change in all we do, including hosting a DERJ Symposium, employee trainings, affinity groups, vendor relations, and a health equity fellowship program for recent graduates.
DERJ Operation Framework
This frame provides the theory of change, which gives us confidence that the proposed activities will yield the desired impact and propel us closer to a more diverse, inclusive, and racially just state.
Human Resources
Reorient Human Resource policies and practices to provide for and assure proportional representation of the population C3 services.
Racial Justice
Support the racial justice movement within the communities we serve and the industry.
Inclusion
Dismantle all forms of racism against Black, Indigenous, and People of Color within C3.
Health Equity
Close health disparity gaps to a variance of less than 5% for each measure.
Medicaid Health Equity Strategic Plan 2023 Summary
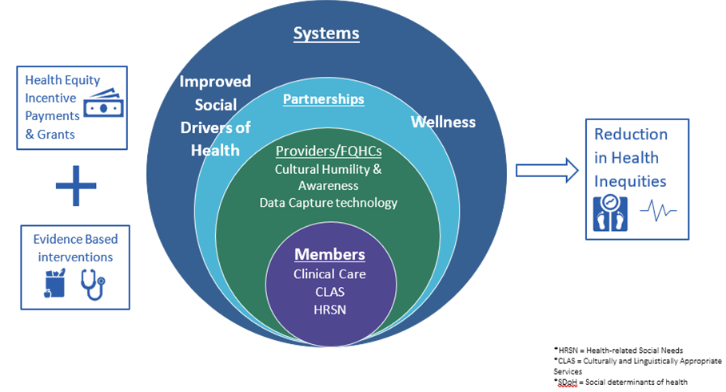
The Social-Ecological Model is a valuable framework for advancing health equity as it considers the multiple levels of influence on health outcomes. This model recognizes that individual behaviors and choices are shaped by the broader social and environmental context in which they occur, including through interpersonal relationships, community norms and values, organizational policies and practices, and larger social, economic, and political systems. By understanding and addressing these various levels of influence, the Social-Ecological Model offers a more comprehensive and holistic approach to promoting health equity.
Over the next four years, our Health Equity Program will address the three prevailing health challenges confronting our ACO. An analysis of our clinical and insurance claims data identified Emergency Department (ED) visits among members with Mental Illness (MI), hypertension, and diabetes as the significant health concerns within our member population. When disaggregated by Race, Ethnicity, and Language (REL), the data revealed a disproportionate representation of Hispanic members among those with MI visiting the ED. Additionally, our Black members showed disproportionately poor outcomes for hypertension while members without self-reported race data had poor outcomes for diabetes.
Due to the unavailability of reliable Disability and Sexual Orientation and Gender Identity (D/SOGI) data, we could not disaggregate data by these demographics. Therefore, our primary focus for the next four years will center on addressing inequities related to race and ethnicity. We plan to address D/SOGI disparities after three years of intensive data collection.
Our strategic goals for the next four years are as follows:
- Goal 1: By the end of 2024, we will increase the percentage of ACO attributed Black members 18-64 years of age who had a diagnosis of hypertension (HTN) and whose BP was adequately controlled (<140/90 mm Hg) during the measurement year by 2% and by an additional 2% every year until 2027.
- Goal 2: By the end of 2024, we will reduce the percentage of ACO attributed members 18–64 years of age with diabetes, who did not provide a valid self-reported race response and whose hemoglobin A1c (HbA1c) level was poorly controlled (>9.0%) by 2% and by an additional 2% every year until 2027.
- Goal 3: By the end of 2027, we will increase the percentage of emergency department (ED) visits for members 6 to 64 years of age with a principal diagnosis of mental illness or intentional self-harm, who had a follow-up visit for mental illness within 7 days of the ED visit by 10%. (This goal will be part of our QHEIP Performance Improvement Plan, which is still in development.)




